The Attendant Who Missed Everything
A 72-year-old in Sector 31, Gurgaon, had a full-time home attendant for three years. The attendant prepared meals, managed medications in a pill organizer, helped with bathing, and filed daily WhatsApp updates with the family: Aunty took breakfast. Blood pressure fine. All ok.
On a Tuesday morning, the family received a call from the building security: their mother had collapsed in the lobby during her morning walk. At the hospital, the diagnosis was acute stroke, the second one in six months. The first had been silent, leaving her with mild speech slurring that the attendant had not flagged as abnormal. The second had been visible, but by then, intervention windows had closed.
The attendant was not negligent. She was untrained in clinical assessment. She knew what to do (medications, hygiene, safety). She did not know what to watch for (subtle neurological changes, cardiovascular warning signs, cognitive shifts). The difference between supervision and clinical monitoring is not just presence, it's precision.
Why Gurgaon's Attendant Model Fails
Gurgaon's model of senior care relies heavily on the home attendant: typically a woman aged 35-60, often migrant, earning Rs. 15,000-25,000 per month, with minimal formal training in geriatric assessment. The attendant becomes the primary interface between your parent's health and the outside world. She is simultaneously cook, nurse, companion, safety monitor, and medication manager, roles that require fundamentally different skill sets.
The problem is structural: we've outsourced care to someone with no clinical training, then act surprised when clinical issues are missed.
In Gurgaon's high-rise model, this creates specific blind spots:
Subtle Neurological Changes: A mini-stroke (TIA), early Parkinson's tremor, or balance shifts go undetected because the attendant has no baseline neurology training.
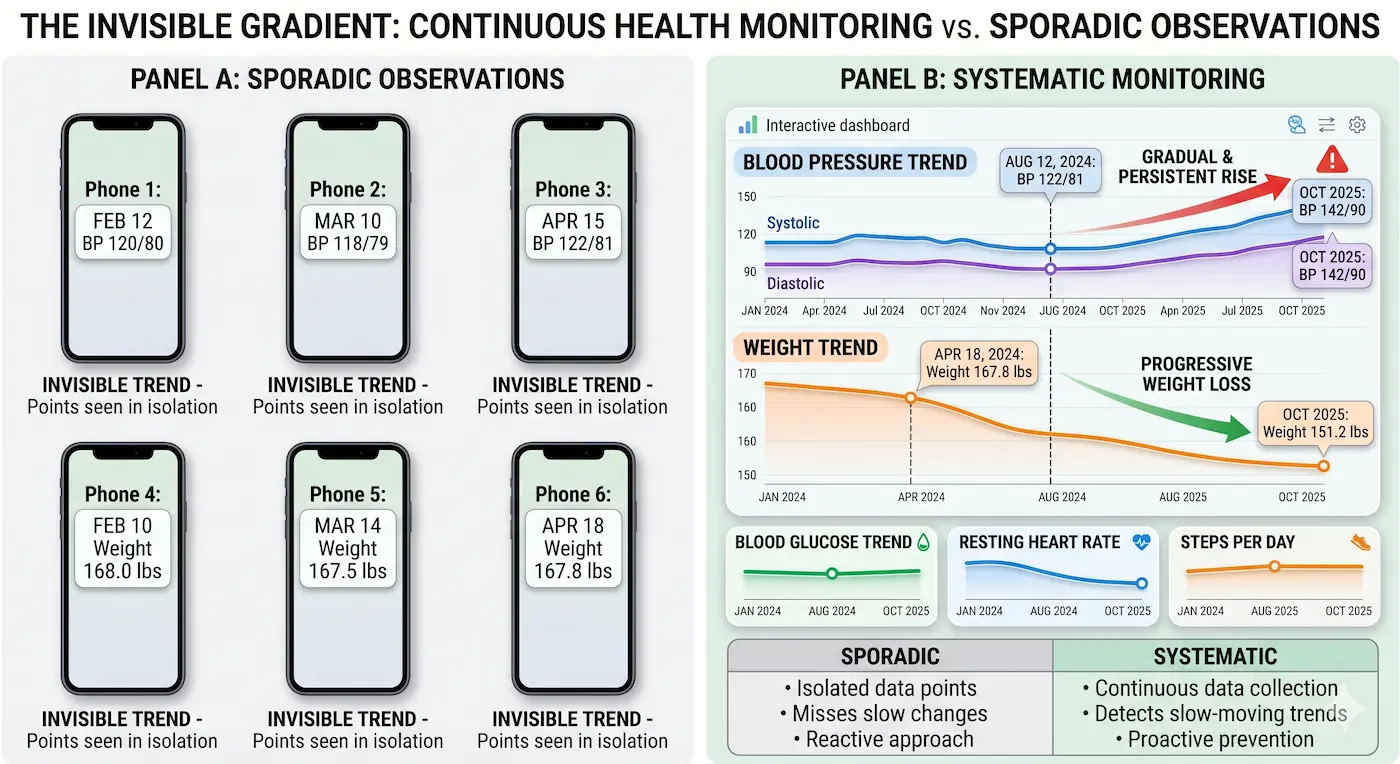
Cardiovascular Drift: Your parent's blood pressure is rising gradually, or they're experiencing silent ischemia (chest discomfort they don't report because they interpret it as indigestion). The attendant takes one reading, notes it down, and misses the pattern.
Medication Interactions: Your parent is seeing three different doctors (orthopedist, cardiologist, general practitioner) and each prescribes independently. The attendant fills the organizer but doesn't flag that Drug A and Drug B interact, or that the new hypertension medication conflicts with existing supplements.
Cognitive Decline: Your parent becomes slightly more forgetful forgetting names, repeating stories. The attendant attributes this to normal aging rather than recognizing early mild cognitive impairment (MCI) that could be slowed with early intervention.
Nutritional Gaps: The attendant prepares familiar foods, but your parent's dietary needs have shifted due to undiagnosed conditions (renal issues, prediabetes, malabsorption). No one flags that they're eating the wrong foods for their current physiology.
Psychological Monitoring: Depression, anxiety, or early confusion manifests as behavioral change. The attendant interprets this as moodiness or stubbornness rather than clinical symptoms requiring assessment.
The Clinical Monitoring Difference: What Actually Gets Caught
Clinical monitoring is not mystical. It is systematic observation against known geriatric risk patterns. Here's what a clinically trained monitor whether a nurse, care coordinator, or physician actually does differently:
Scenario | Home Attendant Response | Clinical Monitor Response |
|---|---|---|
Parent complains of dizziness while standing | Helps them sit down; notes felt dizzy in message to family | Measures orthostatic vital signs (BP lying, sitting, standing); checks medication list for culprits (diuretics, antihypertensives); assesses hydration status; flags if pattern emerges |
Parent forgets appointment or repeats story multiple times | Reminds them; attributes to age | Screens for cognitive decline using validated tools; tracks frequency and severity; distinguishes normal aging from MCI from early dementia; recommends neuropsych evaluation if indicated |
Parent refuses to eat certain foods | Prepares alternatives to ensure compliance | Asks why is it taste change (medication side effect, zinc deficiency), swallowing difficulty (dysphagia), loss of appetite (depression, medication), or digestive distress (reflux, constipation)? Identifies the root cause and adjusts care accordingly |
Parent's ankles are swollen | Notes swelling, mentions in message | Measures circumference at consistent location; checks for pitting edema; assesses if unilateral (clot risk) or bilateral (heart or kidney issue); checks medication list for sodium content; may recommend physician evaluation for congestive heart failure or renal function change |
Parent has fallen at home | Helps them up, ensures no major bleeding | Assesses mechanism of fall; checks for injuries (including subtle ones like rib fractures); evaluates fall risk factors (balance, strength, vision, orthostasis, footwear, home hazards); flags if recurrent, recommends physician evaluation and fall prevention interventions |
Parent seems withdrawn or quiet | Attributes to mood or tiredness | Screens for depression using geriatric-specific depression scale (GDS); assesses for suicidal ideation; checks for medication side effects; evaluates for pain (often expressed as withdrawal in seniors); flags social isolation factors; recommends psychological evaluation if indicated |
The difference is not effort, the attendant works hard. The difference is training in the language of geriatric risk.
The Economic Reality: Why Clinical Monitoring Seems Expensive
Here's the hard math that Gurgaon families often skip:
A home attendant costs Rs. 20,000/month.
A part-time nurse (8 hours/week) costs Rs. 12,000-18,000/month.
A geriatric care coordinator (5 hours/week, remote oversight) costs Rs. 15,000-25,000/month.
A hospitalization for a preventable condition (stroke, fall, medication error, UTI progressing to sepsis) costs Rs. 200,000-1,000,000+.
Families often choose the attendant alone because it looks cheaper. But one missed clinical signal - one silent MI, one undetected infection, one medication interaction erases the savings and adds trauma.
This is the inverse of how we think about car maintenance. We don't skip oil changes to save money on service, we know that skipping service costs more in catastrophic repairs later.
The Clinical Monitoring Toolkit: What Gurgaon Families Actually Need
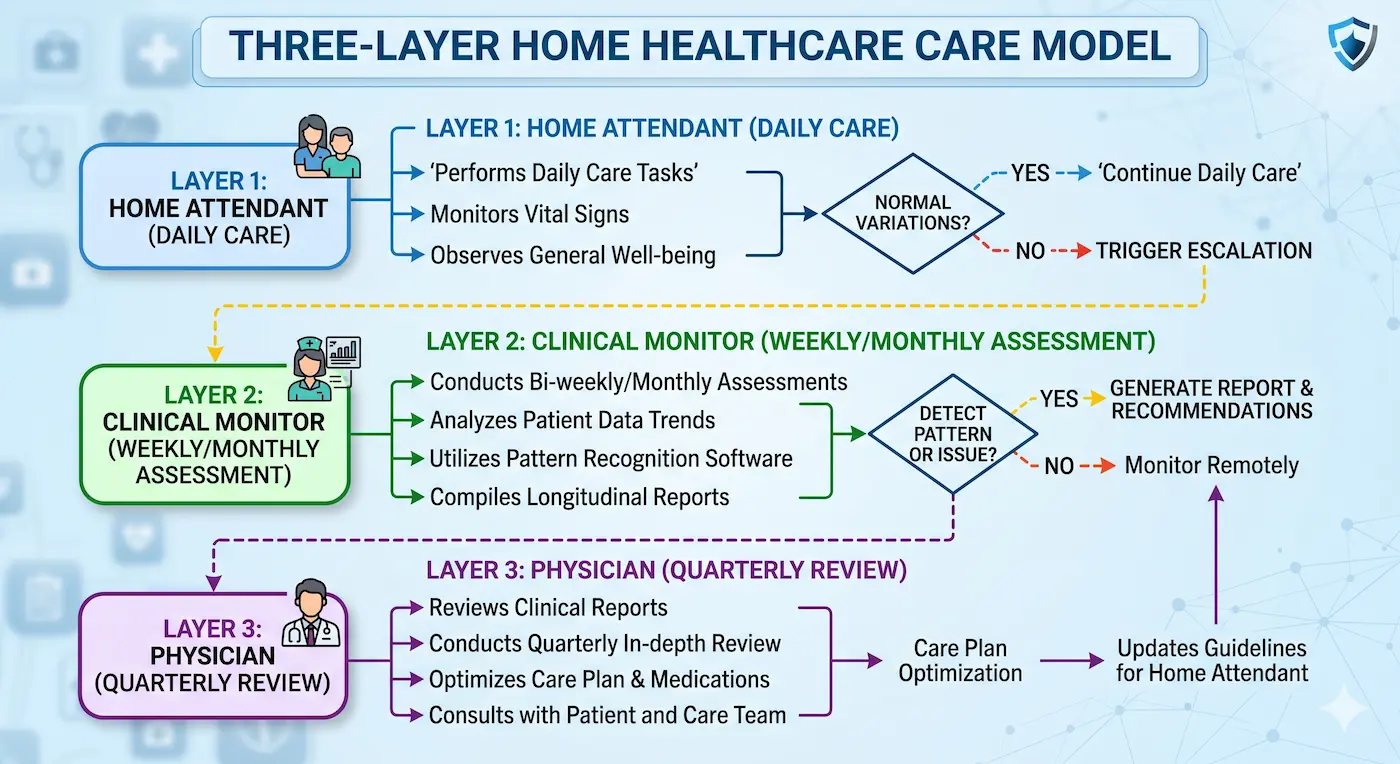
You don't need to replace the home attendant. You need to augment her with clinical oversight. Here's a practical framework:
Layer 1: Structured Baseline Assessment (Month 1)
Arrange for a geriatrician or nurse practitioner to conduct a comprehensive assessment:
Full medication review (checking interactions, appropriateness for age, side effects)
Cognitive screening (MoCA, MMSE)
Mood screening (GDS-15 for depression)
Functional assessment (ADLs, IADLs)
Fall risk evaluation
Nutritional assessment
Cardiovascular risk stratification
Cost: Rs. 5,000-10,000. Done once, it becomes the baseline against which everything else is measured.
Layer 2: Attendant Training (Ongoing)
Brief your attendant on what to watch for. This is not making her a nurse; it's making her a trained observer. Provide a simple checklist:
Daily: Did they eat normally? Sleep well? Seem themselves?
Weekly: Any falls, near-falls, dizziness, confusion, changes in appetite or bathroom habits?
Monthly: Any behavior changes? Mood changes? New complaints?
Provide a simple symptom log template. Train her to describe (swelling where, how much?), not just report (swelling).
Layer 3: Regular Clinical Check-Ins (Monthly or Quarterly)
A nurse or care coordinator reviews the attendant's observations, takes fresh vital signs, and reassesses against baseline. This is the pattern recognition layer.
Cost: Rs. 3,000-5,000 per visit, or Rs. 15,000-25,000/month if structured as ongoing coordination.
Layer 4: Physician Oversight (Quarterly)
Your parent's primary physician reviews the clinical monitor's assessment, runs any indicated labs, and adjusts care plan. This is the decision-making layer.
The Gurgaon-Specific Clinical Monitoring Gap
Gurgaon presents unique challenges for clinical monitoring:
The Doctor Fragmentation Problem: Your parent sees a cardiologist in Sector 14, an orthopedist in Sector 7, and a general physician in their own building. None of them see the full picture. There's no coordination. Clinical monitoring coordinates across specialists.
The Isolation Problem: Your parent lives in a high-rise with security, but actual medical oversight is absent. The building has a clinic, but it's staffed by a nurse for bandage changes, not geriatric assessment. Clinical monitoring fills this gap.
The NRI Child Problem: If you're managing your parent's care from Singapore or the US, you cannot be present for daily observation. Clinical monitoring (especially via a care coordinator) becomes your eyes and ears.
The Attendant Turnover Problem: Attendants in Gurgaon have high turnover (6-18 months average). Each new attendant means loss of institutional knowledge about your parent's baseline. Clinical monitoring creates a consistent record that outlives any single attendant.
Practical Implementation: The Three-Month Protocol
Here's how to transition from attendant-only to attendant + clinical monitoring:
Month 1: Assessment & Education
Hire a geriatric nurse or care coordinator for a comprehensive baseline assessment.
Document findings: medications, cognitive baseline, functional status, risk factors.
Brief your attendant on key observations to track.
Establish a simple daily/weekly symptom log.
Month 2: Pattern Recognition
The clinical monitor reviews attendant observations.
Takes fresh vital signs, repeats key assessments.
Identifies any emerging changes.
Flags anything requiring physician review.
Month 3: Optimization
Physician reviews clinical monitor's findings.
Adjusts medications, adds preventive measures, or initiates new interventions if indicated.
Establishes ongoing schedule: typically monthly monitoring for stable seniors, weekly for those with multiple risk factors.
Total cost for three months: Rs. 30,000-50,000. One prevented hospitalization justifies this investment multiple times over.
Closing remarks
Your attendant is not a nurse. She is a caregiver - essential, capable, but working outside her training. The difference between supervision and clinical monitoring is the difference between knowing what happened (your parent fell) and understanding why (orthostatic hypotension from a new medication, weak quadriceps, poor balance from early Parkinson's, home hazards) and preventing recurrence.
Gurgaon's model of senior care has outsourced presence without ensuring precision. You can change this in your family by adding one layer: regular clinical assessment overlaying daily attendant care. It costs more than an attendant alone. It costs far less than a preventable crisis.
The home attendant keeps your parent safe today. Clinical monitoring keeps them healthy for years.
Signs Your Attendant Is Out of Depth
Do not blame the attendant for these. Blame the system that assigned her clinical responsibilities without clinical training. If you observe any of the following, your parent needs clinical oversight beyond home attendant care:
Medication management confusion: Your parent takes medications but you're not sure if they're being taken correctly (timing, food interactions, dose skipping). The attendant is guessing.
Untracked vital signs: No one is regularly monitoring blood pressure, weight, temperature trends. You get ad-hoc reports, not patterns.
Behavioral changes attributed to personality: The attendant says your parent is more stubborn, angrier, lazier. Clinical possibility: UTI, medication side effect, depression, early cognitive decline.
Fall history: Your parent has fallen once or more, and the response was help them up. No fall risk assessment. No environmental modification. No strength or balance training recommendation.
Medication list mismatch: You're unsure which doctor prescribed what. There's no medication review happening. Potential for serious interactions.
Nutritional drift: Your parent is losing weight, or eating erratically, or complaining of taste changes. No one is assessing whether this is normal aging, medication side effect, swallowing difficulty, or depression.
Cognitive changes glossed over: Forgetting things, repeating stories. But is this normal aging or early MCI? Is it advancing? No baseline. No tracking.
Social and mental health invisible: You have no idea if your parent is depressed, anxious, or isolated. The attendant reports mood, not clinical indicators.
FAQs
Can't my attendant be trained to do what a clinical monitor does?
How do I find a clinical monitor in Gurgaon?
Is clinical monitoring necessary if my parent is healthy and independent?


